
1. When performing any part of the neurological examination you need to know the anatomy and neurophysiology of what you are testing. All reflexes have an afferent and efferent arm (please learn the anatomy of the afferent and efferent limbs of all reflexes you test; neurology becomes a lot easier when you know things).
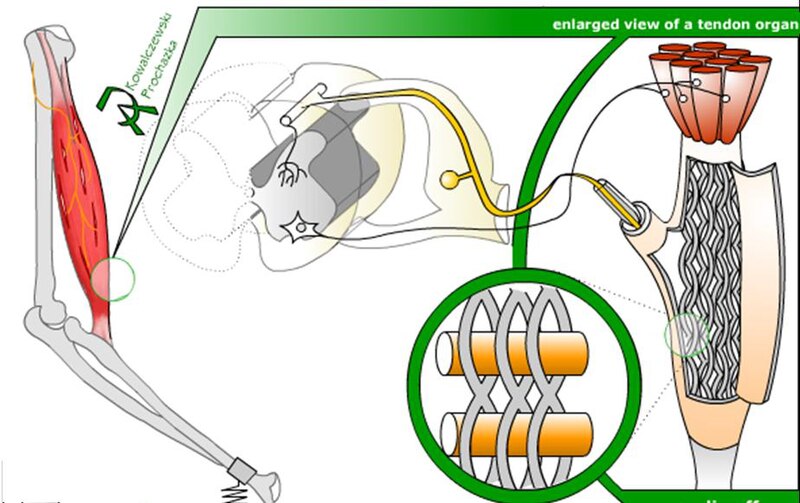
The tendon reflex is a monosynaptic stretch reflex; it is activated by stimulating the golgi tendon organ a stretch receptor. The afferent signal then passes via a large sensory fibre (type Ib), which conducts rapidly (80-120m/sec), to the spinal cord via the posterior roots. A branch of the axon synapses directly on a local population of anterior horn cells to elicit a motor response. Other axonal branches of the Ib sensory axon generates supraspinal responses, via interneurons and ascending tracts, to control muscle contraction and movement (e.g. anterior and posterior spinocerebellar tracts).
2. Know the muscle (tendon) and the corresponding motor root and nerve for each reflex you are testing:
Commonly tested reflexes:
1. Biceps - C5/6, musculocutaneous nerve
2. Triceps - C6/7/8, radial nerve
3. Brachioradialis/supinator - C5/6, radial nerve (please note when you test the brachioradialis reflex you also activate the supinator muscle)
4. Knee jerk - quadriceps muscle, L3/4, femoral nerve
5. Ankle jerk - gastrocnemius and soleus muscle, S1 (minor contribution from L5 and S2), posterior tibial nerve (I was always taught that this was the only reflex that you could quote as having only one root level, i.e. S1)
Less commonly tested:
1. Deltoid - axillary nerve, C5/6
2. Pectoral - medial and lateral pectoral nerves, C5/6 (clavicular head) & C7/8, T1 (sternocostal head)
3. Finger jerks - long finger flexors (flexor digitorum profundus and superficialis), C8/T1, median and ulnar nerves
4. Adductor - hip adductors (longus, magnus,brevis), L2/L3, obturator nerve
5. Hamstring - hamstrings (semitendinosus, semimembranosus, biceps femoris), L5/S1, sciatic nerve
Tip: you may find the the muscle database for nerve and root levels a helpful resource.
3. Which reflex or patella hammer should you use? I am not fussy, but would recommend the Queen Square hammer below. It is flexible and allows you to achieve momentum compared to the short rigid hammers. This makes it easier to use and ensures you are some distance away from the tendon and muscle to observe the motor response.

4. How to do a reflex? Please see the video below. Always compare left and right reflexes with each other. When doing the reflex watch the muscle and limb to see movement. You should also hold the limb in a relaxed way that also allows you to feel the reflex.
"When examining medical students it easy to tell apart students who have practised doing reflexes from those who have not. The neurological examination is like any other skill; you need to do it over and over again until you get good at it."
5. Grading reflexes:
Grade 4: markedly increased, associated with sustained clonus and spread to other muscle groups
Grade 3: increased, associated with non-sustained clonus
Grade 2: easily elicitable
Grade 1: depressed, but elicitable with reinforcement (Jendrassik maneuver)
Grade 0: absent
6. Know what is normal and interpret the reflexes in the clinical context.
All reflex grades described above can be normal. For example, athletes completing the 100m sprint, or someone who has had a fright that has resulted in an increase adrenergic drive, will have increased tendon reflexes, possibly with clonus. These are normal physiological motor responses. Similarly, the elderly will have depressed reflexes and possibly absent ankle jerks (absent ankle jerks are considered normal over the age of 65 in the absence of other neurological signs except reduced vibration sensation to the level of the ankle). Depressed reflexes in the presence of a glove and stocking sensory loss is abnormal and indicates a peripheral neuropathy. Increased tendon reflexes in the presence of pyramidal weakness is a sign of an upper motor neurone lesion. Increased reflexes in association with thyrotoxicosis is due to physiological enhancement of the reflex and is not abnormal. These few examples illustrate that the tendon reflexes need to be interpreted in context; don't jump to premature conclusions before completing the neurological examination and assimilating all information you have at hand.
"I find doing the reflexes after examining the muscle tone, muscle power and sensory modalities most useful. This provides you with information on the afferent and efferent limbs of the tendon reflex before examining and interpreting the reflexes. The classic teaching is to do the tendon reflexes as part of the motor examination, before sensory testing."
Ankle Clonus
Knee Clonus
7. History of the tendon hammer: I would encourage you to read this short piece on the history of the tendon hammer. Danielle Goldberg, a student from Glasgow, wrote it as a library project during her medical elective in July 2010.
No comments:
Post a Comment