
We saw a 68-year old lady on the ward. She had no
past medical history of note.
She presented to hospital with a self-terminating
generalised tonic-clonic (GTCS) and in addition was found to have a dense right
hemiplegia and expressive dysphasia. The presentation was preceded by a 3-4
week history of increasing confusion and disorientation.
On examination she
appeared alert but had significant expressive dysphasia
She was consistently following instructions: 2 and 3 stage
commands. There was a subtle ptosis on the left and unequal pupil size. No
papilloedema. (Horner’s)
There was a small recent Neurosurgical scar in the right
frontal region and a dense right hemiplegia. On further inspection there was wasting
of FDIO on the right as well as heberden’s nodes & mild ulnar deviation of
the digits. On palpation there was arthralgia in small muscles of the hands,
ankle and knee on the right (- ?OA ?RA)
Auscultation of the heart was normal (with normal
echocardiogram) and there were no other systemic features (no fever,
lymphadenopathy or rash)
Differentials based on clinical findings:
Most likely differential is a vasculitic syndrome leading to
ischaemia in the territory of anterior choroidal artery,
MCA or internal carotid artery. VZV vasculitis is in the differential as is primary CNS angiitis
Angiocentric lymphoma
Vasculitis secondary to systemic disease such as rheumatoid
arthritis
PML could cause this but is usually more indolent
Susacs unlikely as there is no history of headache or
hearing deficit
PML would typically follow a more indolent course
Learning points highlighted in discussion of the case:
1. Differentials for
confusion/delirium:
- Drugs
- Dementia
(DLB)
- Infection
(urine and chest most commonly)
- Head
trauma (look for rhinorrhoea, evidence of previous neurosurgery, evidence
- Hypoxia
(ABG)
- Psychiatric
- Seizures
(non-convulsive, may be secondary to either frontal or temporal seizures.
Typically confusion would be fluctuant)
- Space
occupying lesion (papilloedema)
- Metabolic
(Renal failure, Liver failure, electrolyte abnormality)
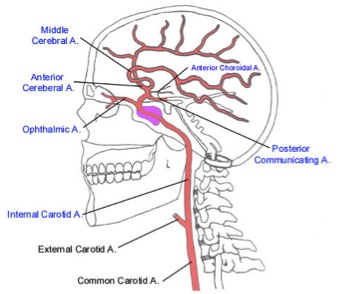
2. The pathway of the
internal carotid artery:
Enters the cranium through the Foramen lacerum, then travels
through the
Cavernous sinus. It then turns to travel under the anterior
clinoid process emerging just below and posterior to the optic canal. The
internal carotid artery finally emerges through the dura just beneath the optic
nerve.
There are 5 terminal branches: MCA, ACA, ophthalmic,
posterior communicating and anterior choroidal artery. The ophthalmic artery
supplies the contents of the orbit and continues forward to supply the central
part of the forehead.
3. Syndromes related
to anterior choroidal artery infarction
Most commonly patients present with a lacunar syndrome (85%)
but there are case studies of confusion and aphasia, presumably where the superficial
territory is involved, leading to cortical deficits.
Further reading: Palomeras E, Fossas P, Cano AT,
Sanz P, Floriach M. Anterior choroidal artery infarction: a clinical, etiologic
and prognostic study. Acta Neurol Scand 2008: 118: 42–47
4. Horner syndrome
Classically the patient will have ptosis, miosis and
anhidrosis. There may be mild enophthalmos secondary to lid sagging. There is
also increased amplitude of accommodation. Acute features of sympathetic
disruption include ipsilateral conjunctival injection and nasal stuffiness.
The precise clinical manifestation depends upon the site of
the lesion along the three-neuron sympathetic (adrenergic) pathway, that
originates in the hypothalamus:
- 1st
order neuron: descends caudally from hypothalamus to the first synapse located
in the spinal cord (levels C8-T2). Causes include stroke, demyelination,
pituitary or base of skull tumours, basal meningitis, neck trauma,
syringomyelia, Arnold chiari malformation and spinal cord tumours.
- 2nd
order neuron: travels from sympathetic trunk, through the brachial plexus, over
the lung apex and ascends to the superior ganglion, located near the angle of
the mandible and bifurcation of the common carotid artery. Causes include
apical lung tumours (eg. Pancoast’s), lymphadenopathy (lymphoma, leukaemia,
TB), lower brachial plexus trauma, common carotid or subclavian aneurysm,
neuroblastoma or mandibular dental abscess.
- 3rd
order neuron: ascends within the adventitia of the internal carotid artery,
through the cavernous sinous in close relation to CN VI. The oculosympathetic
pathway then joins V1. In the orbit the fibres innervate the iris dilator
muscle as well as Muller’s muscle (responsible for a small proportion of upper
lid elevation and lower lid retraction). This innervation accounts for the
minor ptosis (<2mm). Anhidrosis is not a feature of 3rd order
lesions as the sympathetic fibre responsible for sweating and vasodilation
branch off at the superior cervical ganglion. Causes include cluster headache
or migraine, herpes zoster infection, internal carotid artery dissection,
carotid-cavernous fistula and temporal arteritis.
Neurological signs can help to localise the lesion:
diplopia, vertigo, ataxia, lateralised weakness à Brainstem
bilat/ipsilat weakness, long tract signs, sensory level,
bladder or bowel involvement à
Myelopathy
Arm pain/weakness à
brachial plexus or lung apex
Ipsilateral ocular paresis & CN VI palsy, no brainstem
signs à cavernous sinus
Isolated honers with neck pain àinternal
carotid artery dissection
5. Neurological
manifestations of rheumatoid arthritis
Manifestations may be either central or peripheral and
related to the disease itself or disease modifying treatment.
CNS manifestations: cervical myelopathy (secondary to
atlantoaxial subluxation), vasculitis, rheumatoid nodules within the CNS,
meningitis and rarely progressive multifocal leucoencephalopathy (risk
increased after rituximab therapy) and a hyperviscosity syndrome. Stroke also
occurs with increased frequency
PNS manifestations: compression neuropathies (most common,
secondary to joint deformities, inflamed synovium, ligaments or compressive
tendon sheaths), distal sensory neuropathy, sensori-motor neuropathy or
autonomic neuropathy (thought to be secondary to vasculitic process)
Neuromuscular manifestations: myopathy, disuse atrophy,
denervation atrophy, myositis.
RA may rarely be complicated by secondary amyloidosis.
Drugs effects:
●Nonsteroidal antiinflammatory drugs (NSAIDs) à headaches, drowsiness, and aseptic meningitis
●Glucocorticoids à
myopathy, depression, psychosis & intracranial hypertension
●Gold à peripheral neuropathy,
cranial nerve palsies and Guillain-Barré syndr
●Methotrexate, Sulfasalazine and leflunomide à headaches.
●Leflunomide àperipheral neuropathy
● anti-TNF therapies à increase
the risk of demyelinating disease
No comments:
Post a Comment